This week the review covers studies on various diet plans and two papers on breast cancer prevention. The take home message has to be that macronutrient combinations are less important than the overall quality of the diet and fibre intake is a good measure of diet quality with plenty of benefits for health. It’s certainly not a great week for low-carb/keto diet advocates!

WHICH DIET IS BEST FOR WEIGHT LOSS AND CARDIOVASCULAR DISEASE (CVD): Selling diet plans is a multi-billion pound industry, so it’s important to have evidence to help consumers make the right decision. This study reports the outcome of 121 trials using a number of popular diet programmes and focusses on the impact of different macronutrients combinations on weight loss and CVD risk factors at 6 and 12 months follow-up. It should be noted that the the comparisons between diets included are subject to bias and hence the level of evidence in the paper is considered low. The summary of the results are shown in the table below taken from the paper.
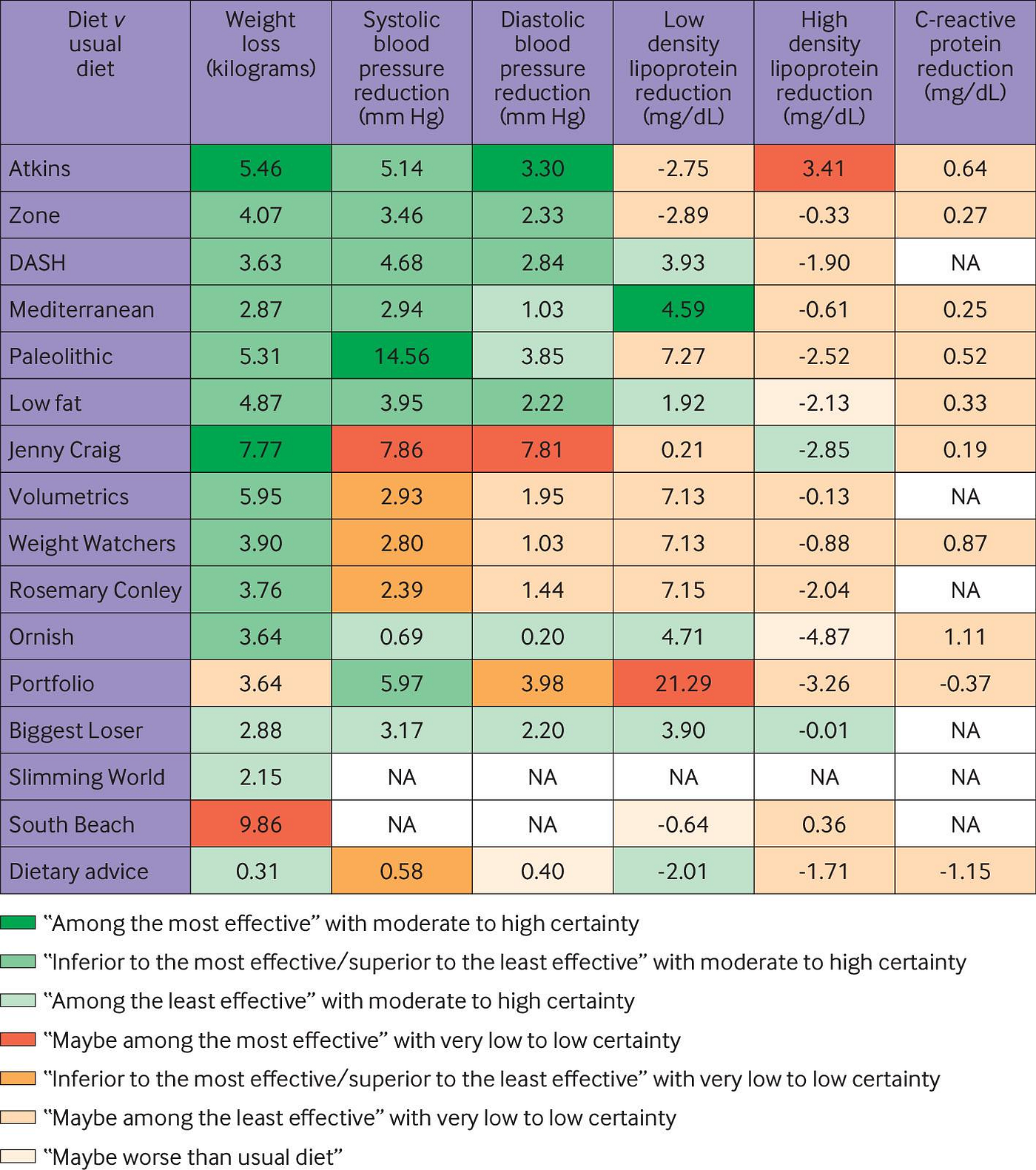
Overall, the results show that there is very little difference in outcome of the various diet programmes at 6 months with most of the benefit lost by 12 months. Most diets reduced weight and improved CVD risk factors at 6 months with some small differences between low-carb and low-fat diet patterns. The only diet pattern that retained some benefit at 12 months was the Mediterranean diet. The take home message has to be that we have to move away from using popularised diets to improve health and concentrate on eating healthy foods. People choose foods and not macronutrients and therefore the focus should be to encourage healthy foods choices. In addition, maintaining weight loss requires a different focus with sustainable diet choices coupled with physical activity. As stated in the accompanying editorial ‘As national dietary guidelines fail to resonate with the public, taking a food based approach with individuals and encouraging them to consume more vegetables, legumes, and whole grains and less sugar, salt, and alcohol is sound advice’.

WHICH DIET IS BEST FOR OPTIMISING BLOOD PRESSURE (BP) IN PATIENTS WITH TYPE 2 DIABETES (T2D): This study again examines the impact of a variety of diet plans, but this time on systolic and diastolic BP. The meta-analysis includes 24 randomised controlled trials, including 1130 T2D patients, and compares 11 different dietary approaches (DASH, Low-fat, Low-carbohydrate, High-protein, Low-protein, Mediterranean, Paleolithic, Vegan, High-fibre, Low-GI/GL, Low-sodium, and Korean-traditional).
Compared to a control diet, a number of dietary interventions were effective at lowering BP. A Low-sodium diet was the most effective dietary approach for reducing SBP, followed by the High-fibre, and the DASH diet. High-fibre diet was the most effective dietary approach in reducing DBP, followed by the Low-fat and Low protein diet. The Low-sodium, High-fiber, DASH, Low-fat, High-protein, Low-protein and Vegan dietary approach were significantly more effective in reducing SBP (10.84 to 3.05 mmHg) compared to a control diet. The High-fibre, Low-fat, Low-protein and Vegan diet were significantly more effective in reducing DBP (7.28 to 3.1 mmHg) in comparison with a control diet. Low-sodium diets do not reduce DBP (consistent with previous findings). Low-carb and Paleo diets in this analysis had no significant effect on BP in patients with T2D, although there is some inconsistency with previously published studies. Overall, for reducing both SBP and DBP, the High-fibre diet came out top.
From the data presented and without analysing each study included (which I have not done!) it is difficult to tease out the exact definition of each of these diet plans, whether the trials involved calorie restriction and whether participants also lost weight. Nonetheless, a low-sodium, high-fibre diet is sound advice for patients with T2D.

KETO DIETS NOT SO GOOD: Three reports of the potential hazards of a ketogenic diet, an extreme version of a low-carbohydrate diet, are highlighted. The first study examined the pattern of symptoms, severity and time course of headache, fatigue, nausea, and other symptoms referred to as the ‘keto flu’ by users of online forums. The commonest symptoms reported in >10% of online post were flu, headache, fatigue, nausea, dizziness, brain fog and gastrointestinal discomfort. These symptoms occurred in the first 4 weeks. The most commonly suggested remedies included increasing intake of various electrolytes such as sodium, magnesium and potassium, suggesting that nutritional imbalances may be contributing to these symptoms.
This second study investigated the effects of a keogenic diet on muscle fatigue in healthy, young, and women of normal weight. Twenty-four women were randomised in a crossover design study to a 4-week ketogenic followed by a 4-week control diet or the reverse sequence. Treatment periods were separated by a 15 week washout period. Seventeen women completed the study and were included in the analyses. After 4 weeks, the ketogenic diet had no effect on grip strength or time to fatigue, a measure of peripheral muscle fatigue. However, the time to reach exhaustion on the cycling test was significantly reduced after 4 weeks on a ketogenic diet. Participants’ own diary notes reported that they found daily life activities more strenuous and were more fatigued during exercise. This study suggests that in young and healthy women, a ketogenic diet has a negative effect, certainly in the short-term, on muscle fatigue and might affect perceived exertion during daily life activities.
This third paper is an opinion piece and is hypothesis generating. The paper reminds us how glucose can result in vascular damage by binding to an amine in protein to form advanced glycation end products (AGEs). AGEs bind to their receptor, RAGE, found on vascular endothelial and smooth muscle cells and macrophages, which results in inflammation, vascular damage and atherosclerosis. Ketones can also react with proteins, modifiying their structure and making them into a ligands for RAGE — i.e. they bind and activate RAGE. This may then also result in inflammation and vascular damage. This hypothesis could explain the increased mortality associated with low-carb diets in the longer term.

I appreciate that all 3 papers highlighted would not be considered high quality research but they add to the observational data, which suggests a low-carb/ketogenic diet can adversely affect health outcomes in the long term.
FIBRE CONSUMPTION AND BREAST CANCER: A significant proportion of breast cases are preventable through healthy lifestyle behaviours. A healthy diet is paramount. This meta-analysis, including 20 prospective studies, mostly cohort studies, confirms that dietary fibre has a significant protective effect against the development of breast cancer. A high total fibre intake reduced the risk by 8% with soluble fibre conusmption (dried beans, oats, oat bran, rice bran, barley, citrus fruits, apples, strawberries, peas, and potatoes) having a greater effect than non-soluble and reducing the risk by 10%. All sources of fibre — fruits, vegetables, cereals and legumes — seem to be beneficial with perhaps fruit fibre having a greater effect. Fibre consumption really reflects a good quality diet. Fibre helps maintain a healthy weight, promotes insulin sensitivity, maintains a healthy gut microbiome and hence immune system and reduces blood levels of cholesterol and oestrogen.
In the UK, the average daily consumption of fibre is 19g when we really should be aiming for at least 30g a day. The only sources of fibre are whole plant foods which the UK diet is certainly lacking in.

GREEN TEA AND BREAST CANCER: The clinical literature on the impact of green tea consumption on breast cancer risk has been inconsistent to date. Certainly in the laboratory, the proposed active compound epigallocatechin 3-gallate (EGCG) can inhibit breast cancer cell growth and induce cell death. The aim of this meta-analysis was to assess the dose-response of green tea consumption on breast cancer risk. 16 papers were includes; 7 cohort and 9 case-control studies. 9 of these studies were included in the dose-response analysis. The results show that high green tea consumption may reduce the risk of breast cancer by 14%. The dose-response analysis suggests that long-term, high dose green tea consumption has a protective effect. Drinking one, two, three, five or seven cups of green tea per day, the risk of breast cancer is reduced by 3%, 6%, 8%, 13% and 18%, respectively. However, the impact appears to be mainly on pre-menopausal breast cancer risk, whereas there was a non-significant increased risk for post-menopausal breast cancer. This study certainly does not provide the final answer to this question, and no single food or drink is going to be the key to cancer prevention. Nonetheless, the data as we have it so far suggests that drinking green tea can be a worthwhile component of a healthy diet and may have some action on preventing breast cancer.
For further information in-depth information on breast cancer prevention, read my article here.
If you have found this article useful, please follow my organisation ‘plant-based health professionals UK’ on Instagram @plantbasedhealthprofessionals and facebook. You can support our work by joining as a member or making a donation via the website