A review of the week’s plant-based nutrition news June 14th 2020
This week we have bold and clear recommendations from the American Society of Cancer on diet & physical activity for cancer prevention. I have chosen some studies to complement the guideline. I also highlight inequalities in access to healthy food in the UK.
GUIDELINES FOR CANCER PREVENTION: We know that more than 40% of cases of cancer could be prevented through diet and lifestyle modification. Back in 2018, the World Cancer Research Fund produced comprehensive guidance on steps we should all be taking to reduce the risk of cancer. These recommendations are increasingly important for cancer survivors too. Now the American Cancer Society have updated the guidance, emphasising the importance of personal behaviours but also the responsibility of communities, societies and policy makers to create the right environment for all of us in society to be able to make these healthy choices for ourselves and our families.
The emphasis is very much on a healthy diet pattern rather than individual foods and nutrients. A healthy diet pattern not only excludes carcinogens and includes foods that protect against cancer, it also helps maintain a healthy weight. Obesity continues to be a significant cause of cancer, second only to tobacco smoking. A healthy diet pattern is considered one that is based around whole plant foods — fruits, vegetables, whole grains and legumes. It limits or avoids red/processed meat, sugar-sweetened beverages and processed foods. So a healthy diet pattern could be a vegan or vegetarian diet, the Mediterranean diet, the DASH diet and one that is consistent with the Alternate Healthy Eating Index.
With regards to supplements, the only one for which there is some evidence, albeit inconclusive, is vitamin D. Based on the available data, it is well worth taking a supplement to keep blood levels in the normal range if sun exposure is not adequate
The guideline has been bold in stating that for cancer prevention DO NOT drink alcohol as there is no safe limit. No type of alcohol beverage is less risky in terms of its impact on cancer risk. Alcohol consumption is the third major modifiable cancer risk factor after tobacco use and excess body weight. The good news is that coffee may be associated with a reduced risk of certain cancers.
The guideline also addresses the evidence around several commonly asked questions. Acrylamide is found in food and formed as a by-product of the Maillard reaction, in which the amino acid asparagine reacts with certain sugars when heated to high temperatures. The major sources of acrylamide in our diets are French fries and potato chips; crackers, bread, and cookies; breakfast cereals; canned black olives; prune juice; and coffee. Although classified as a ‘probably carcinogen’ in humans there is no strong evidence that dietary acrylamide exposure is associated with the risk of any type of cancer. Try to reduce exposure to arsenic in food and water. Foods known to contain high levels of arsenic, including seafood, rice and rice products, and fruit juice. Maintaining good folate status is important for the elimination of arsenic in the body. Although not a specific concern here in the UK, at present there is no evidence that genetically modified crops increase the risk of cancer. There is no evidence to support a gluten-free diet for cancer prevention, unless you have coeliac disease, and gluten-containing whole grain consumption is associated with a lower risk of colorectal cancer. There is currently no evidence that irradiation of food causes cancer or has harmful effects on health. There is no scientific evidence to support claims that exclusively consuming juices for ≥1 days reduces cancer risk or provides other health benefits. Microwave cooking does not increase the risk of cancer. Contamination of foods by substances from storage containers or cookware is another concern. This relates mainly to plastic containers and Teflon-coated cookware. The link with cancer is inconsistent. Until we have more evidence, it may be wise to choose glass or metal storage containers and cookware. There is no clear evidence that artificial sweeteners, at the levels typically consumed in human diets, cause cancer, although they are not considered necessary or healthy per se. Choosing organic produce over non-organic may reduce the risk of non-Hodgkin lymphoma but it is important for individuals with limited resources to recognize that meeting the recommendation for vegetable and fruit intake is a higher priority for cancer prevention and overall health than choosing organic produce. Washing conventionally grown produce can remove some of the pesticide residues, and is also important to minimize the risk of microbial contamination. Adequate and good quality sleep is important for cancer prevention. Soya foods may be beneficial for prevention of cancers such as breast and prostate cancer, but soya supplements should not be used.
The final paragraph states ‘Many studies of vegetarians (this includes vegan diets!) indicate a lower risk of cancer overall relative to people who also eat meat……vegetarian dietary patterns are associated with a lower risk of cardiovascular disease and type 2 diabetes and are generally more affordable’.


RED AND PROCESSED MEAT, COOKING METHODS AND COLORECTAL CANCER RISK: In 2015 the WHO classified processed and red meat consumption as group 1 (causes cancer) and group 2a (probably causes cancer) carcinogens. This was in relation to a colorectal cancer (CRC). The risk is related to compounds in the meat itself and also chemicals produced with high heat cooking — mutagens (damages DNA) such as heterocyclic amines and polycyclic aromatic hydrocarbons. CRC can be derived from colonic polys of which there are 3 types. This case-control study with 7621 participants examined the impact of red/processed meat consumption, cooking methods and degree of ‘well doneness’ on the risk of one type of polyp — sessile serrated lesion (SSL). Intakes of meat were converted to inferred meat-derived mutagens based on the amount of meat intake and the usual level of meat well-doneness using the software CHARRED created by the National Cancer Institute
The results showed that higher intakes of total meat, red meat, processed meat, well-done meat, well-done red meat, and well-done processed meat were associated with an increased risk of SSLs. This risk was double or triple the risk in those that consumed the most compared to the least. This risk was particularly associated with the intake of the mutagen 2-amino-3,8-dimethylimidazo[4,5-f]quinoxaline (MeIQX) —a heterocyclic amine. The overall intakes of red and processed meats were slightly more strongly associated with SSL risk than well-done intakes of these meats, suggesting that it may not be well-doneness per se that is responsible for the increased risk. Other mechanisms in addition to the generation of carcinogens on cooking, include the presence of haem iron and N-nitroso compounds.
This study adds evidence for the increased risk of CRC with consumption of red and processed meat, with some but not all of this risk related to generation of carcinogenic compounds with cooking.
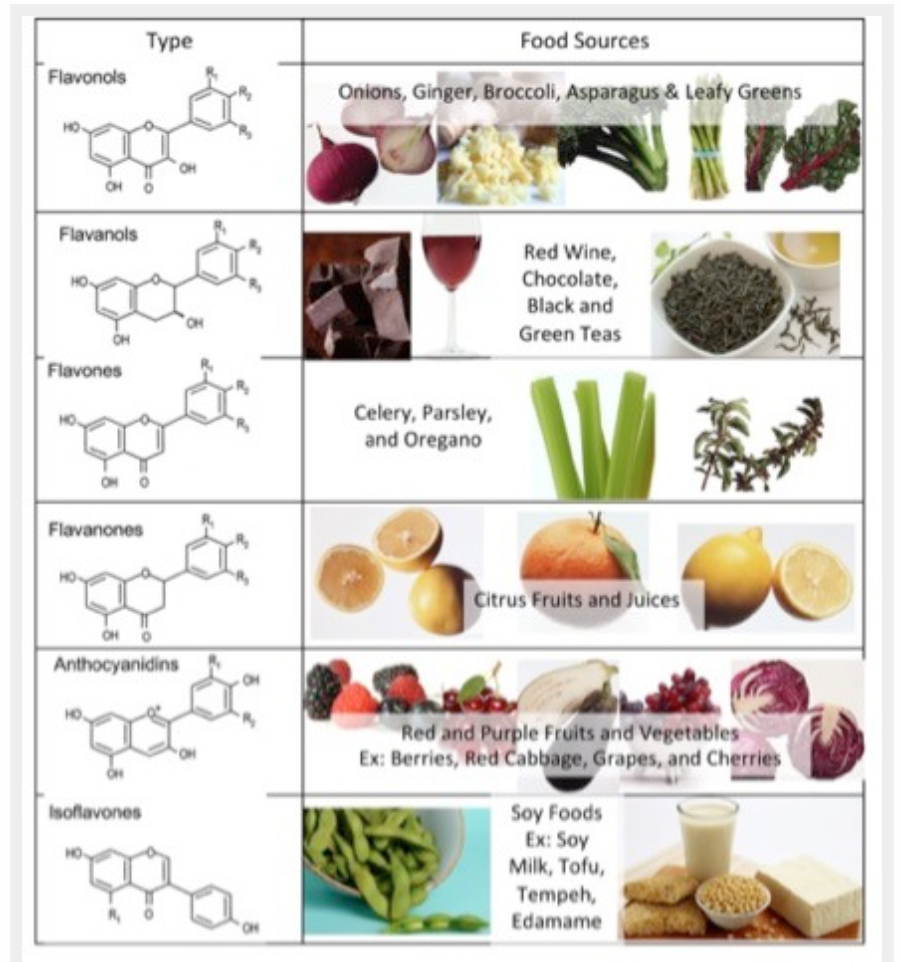
BENEFITS OF FLAVONOID CONSUMPTION: Although its best to concentrate on the overall diet pattern and not individual nutrients, consumption of flavonoids do seem to be associated with improved health outcomes in a large number of studies. Of course flavonoid-rich foods are mainly fruits and vegetables and therefore their intake reflect a healthy diet pattern.
This large study analysed flavonoid intake in 56,468 participants, without cancer prior to enrollment, between the age of 50–65 years, recruited into the Danish Diet, Cancer, and Health cohort study (an associated cohort of the European Prospective Investigation into Nutrition and Cancer) between 1993–97.
The results showed that an achievable dietary intake of total and individual flavonoid subclasses was associated with a lower risk of all-cause, cardiovascular disease (CVD)-related, and cancer-related mortality; in the order of 10–20% risk reduction. The associations were strongest for current smokers and individuals with high alcohol consumption. Results indicated that for total flavonoid intake, risk of all-cause and CVD mortality was lower for flavonoid consumption until intakes of approximately 500 mg/d, after which higher intakes provided no added benefit. This threshold was higher, approximately 1000 mg/d, for cancer-related mortality. These levels are easily achievable through diet with one cup of tea, one apple, one orange, 100 g of blueberries, and 100 g of broccoli being able to provide most of the flavonoid subclasses and over 500mg of total flavonoids. The study population mostly achieved flavonoid intake through consumption of tea, chocolate, wine, apples, and pears.
Plant-based foods contain a wide range of bioactive nutrients. These nutrients are extremely powerful for maintaining health and this study shows they can even counteract some of the negative effects of unhealthy habits — smoking and drinking alcohol!

SURVIVAL AFTER BOWEL CANCER: This study is from the special issue on cancer and nutrition from the British Journal of Nutrition. We already know that predominantly plant-based diets before and after a diagnosis of colorectal cancer may improve remission and survival. Phytooestrogens may be protective against cancer. There are 2 main sources of phytooetrogens in the diet; plant-derived lignans found in whole grains, fibre-rich vegetables and flax seed and isoflavonoids mainly found in soya foods. When plant lignans are ingested, they are converted into primarily enterolactone by the gut microbiota. Therefore, the circulating level of enterolactone depends on the intake of lignans and on the capacity of the gut microbiota to convert plant lignans to mainly enterolactone.
This study reports findings from the Danish cohort study ‘Diet, Cancer and Health’. It includes prediagnosis plasma samples and lifestyle data, and clinical data from time of diagnosis from 416 women and 537 men diagnosed with colorectal cancer. Enterolactone was measured in plasma and use of antibiotics, which can alter gut microbiota and affect the production of enterolactone, was also determined.
The results are summarised in the recently produced video below
A previous study from the same cohort suggests that higher levels of enterolactone in the blood may reduce the risk of endometrial cancer and colorectal cancer in women but not men. It is not clear why there are differences in outcomes for men and women. The adverse outcome for men in the current study was found only among those with 0–5 years between blood sampling and diagnosis, suggesting the disease may have affected the plasma enterolactone concentration. Of note, the positive association in women was only apparent in those that had not used antibiotics prior to blood sampling.

DIET QUALITY AND SOCIOECONOMIC STATUS IN THE UK: Recent weeks have highlighted the socioeconomic disparities in health outcomes in high income countries and the particular impact on ethnic minority communities. This study highlights the issue of access to healthy foods based on socioeconomic status as assessed by education, occupation and income. The study analyzed data on 6416 subjects aged 18 and older collected in the UK National Diet and Nutrition Survey (NDNS 2008–2016). 90% of participants were white with a median age of 48 years. It analysed diet data using the DASH diet score. As previously discussed, the DASH diet was designed around the benefits of the vegetarian diet but includes some low fat dairy and lean meats to be ‘more acceptable’ than the so called ‘restrictive’ vegetarian diet! Nonetheless, it is a plant strong diet pattern associated with improved cardiovascular outcomes in clinical studies.
The results showed that 1 out of 4 people were obese and 1 out of 3 overweight, with little change over the time period studied. The proportion of individuals with no qualification significantly decreased and household income tended to increase over the period. Overall, adherence to a healthy diet is low in the UK but the quality of diet improved in all socioeconomic groups over the time period studied. However, diet quality remained worse in those participants from lower socioeconomic groups. This difference was mainly due to a lower intake of fruit, vegetables, whole grains, nuts, legumes and seeds.
This study adds to prior literature demonstrating the association of socioeconomic status with healthier diet pattern. Those who earn a higher income eat more fruits and vegetables and consume more fibre and eat less processed meat and foods.

The 10 year update to the Malmot review was published in February 2020 and does not make happy reading. People in the UK can expect to spend more of their lives in poor health. Improvements to life expectancy have stalled, and declined for the poorest 10% of women. The health gap has grown between wealthy and deprived areas. Living in a deprived area of the North East is worse for your health than living in a similarly deprived area in London, to the extent that life expectancy is nearly five years less. We have to do better. Healthy food needs to be accessible and affordable for all in society regardless of income.
In the opinion piece highlighted above the author states we need to ‘shift some substantial fraction of health expenditures from an overbuilt, high-priced, wasteful, and frankly confiscatory system of hospitals and specialty care toward addressing social determinants instead’. Only then will we truly benefit the health of all people and communities.
If you have found this article useful, please follow my organisation ‘plant-based health professionals UK’ on Instagram @plantbasedhealthprofessionals and facebook. You can support our work by joining as a member or making a donation via the website