A review of the week’s plant-based nutrition news 5th September 2021
This week, once again, I cover reviews and studies on cardiovascular disease. This is an area of health where there is absolutely no doubt that a plant-predominant diet is the optimal choice. The evidence just keeps accumulating.
NEW GUIDELINES ON CARDIOVASCULAR DISEASE (CVD) PREVENTION: These comprehensive guidelines have just been published. There is a lot of useful information and I encourage you to read the full document (although it is 111 pages!). I have picked out the relevant nutrition advise, but of course a whole lifestyle approach to CVD prevention is hugely important. The guideline acknowledges that as much as 90% of the risk of atherosclerotic CVD, which includes heart attacks, strokes and peripheral arterial disease, can be explained by smoking, poor eating habits, lack of physical activity, abdominal obesity, high blood pressure, raised blood lipid levels, diabetes, psychosocial factors, or alcohol. The recommendations are applicable for healthy adults and those with established CVD or diabetes, which is a major risk factor for CVD. The purpose of the recommendations are to avoid the main risk factors for CVD, which are high blood pressure, high blood lipids, overweight and obesity and type 2 diabetes.
The diet recommendations are clear. A healthy diet is one that is abundant in fruits, vegetables, whole grain, beans, nuts and seeds. A Mediterranean diet pattern is specifically recommended based on the fact that we have the most supportive data on this type of diet pattern. The specific recommendations are shown in the table below.
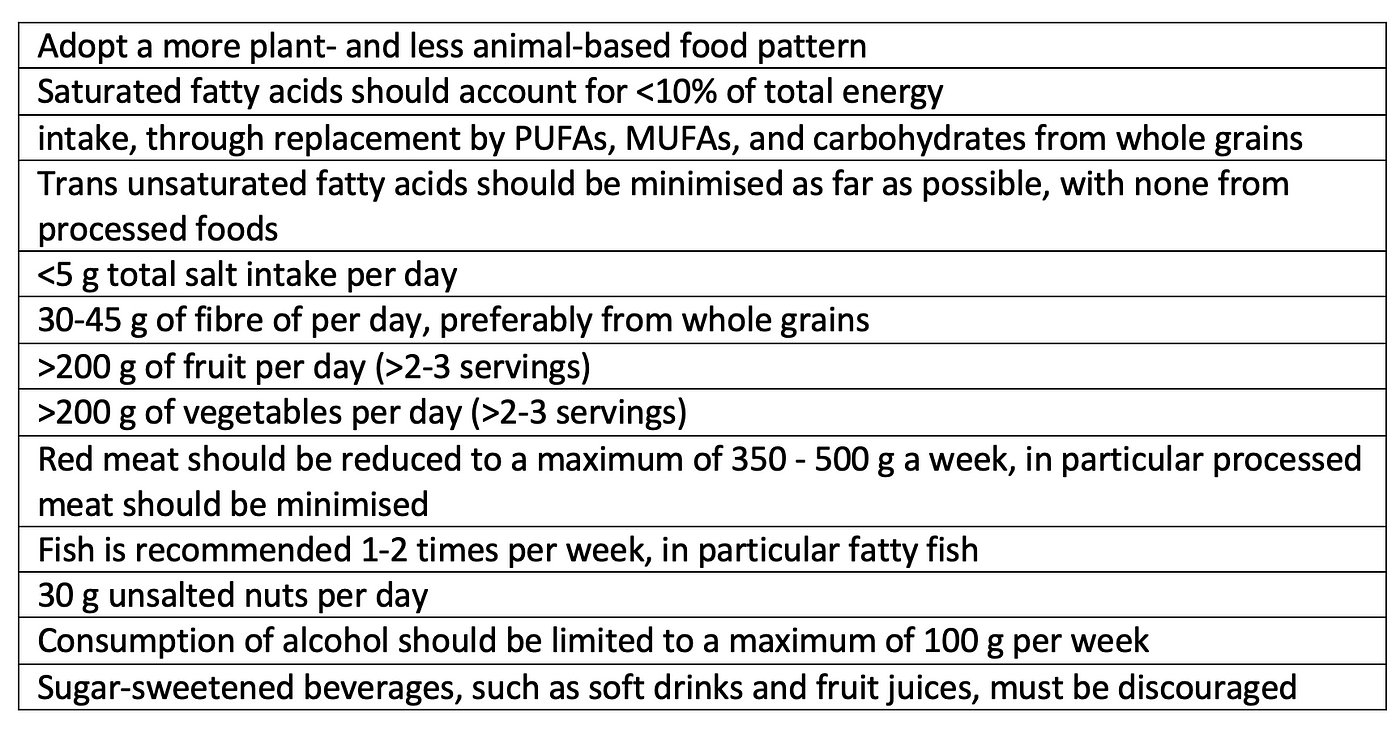
Some points of interest. The recommendations for alcohol consumption seem to have come full circle with initially alcohol (particularly red wine) thought to be protective but now the guidelines state the following ‘Mendelian randomisation studies do not support the apparently protective effects of moderate amounts vs. no alcohol against atherosclerotic CVD, suggesting that the lowest risks for CVD outcomes are in abstainers and that any amount of alcohol uniformly increases blood pressure and BMI. These data challenge the concept that moderate alcohol consumption is universally associated with lower CVD risk’.
The last couple of weeks I have reported on studies that suggest moderate amounts of alcohol may be beneficial for prevention of lupus and the polyphenols in red wine may benefit gut health. I worry about these recommendations in light of the very narrow therapeutic window for alcohol and this is now emphasised by the current CVD prevention guideline.
Regarding the carbohydrate debate the guideline states the following ‘Extreme carbohydrate intakes should be avoided in the long term and plant substitutions of fat and protein for carbohydrates are advantageous over animal ones’. Thus the recommendations mean that if you are going to lower carbohydrate intake this is best done with replacement by plant sources of fat and protein. The guideline is clear that plant-based diets are superior for heart health compared to diet patterns high in animal-based foods and thus saturated fat.
I am disappointed that the guidelines specifically recommend the consumption of fish, specifically fatty fish because of the long-chain omega-3 content, twice a week. There is no doubt that eating fish in place of meat is beneficial for heart health, but there is no evidence to support that fish adds further benefits to an already healthy plant-based diet. This recent Cochrane review comes to this same conclusion. Some studies (although not all) have even shown a mortality advantage when fish is swapped for plant sources of protein. When examining the active components of the Mediterranean diet pattern, fish was not found to be a crucial component, and may even have a negative effect. In addition, reanalysis of the PREDIMED study data (the most famous and widely cited study of a Mediterranean diet) using the pro-vegetarian score (which gives positive scores to all plant-based foods and negative scores to all animal-derived foods) showed a mortality advantage, something the original analysis was not able to demonstrate. When considered with the sustainability aspects of fish consumption and that the recommendations are just not possible without harming our oceans for a predicted population of 10 billion by 2050, my personal opinion is that fish is best left off the plate.
Vegetarian (nor vegan) diet patterns are not mentioned in the document. This is surprising to me given the consistent data we have that vegetarian diets significantly reduce the risk of ischaemic heart disease and mortality. I accept that for a fully vegan diet we need more long-term data. In contrast, the American College of Cardiology 2019 guidelines for primary CVD prevention do highlight the benefits of a vegetarian diet pattern.
Overall, these guidelines provide strong emphasis and reinforcement for the impact of healthy lifestyle habits for the primary and secondary prevention of CVD.

RED MEAT VERSUS ALL OTHER SOURCES OF PROTEIN: Given the cardiovascular theme this week, I thought it was worth highlighting this study from 2019. There still seems to be some level of confusion amongst health professionals about the impact of red meat consumption on health. Some of the strongest evidence we have for eliminating red meat from the diet is the negative impact it has on cardiovascular health, which includes raising blood cholesterol levels. Blood cholesterol is the most important risk factor for CVD. Yet the confusion arises because some studies do not take into account what replaces red meat in the diet when it is removed.
This paper asks some very relevant questions. What happens to CVD risk factors when red meat is removed from the diet and replaced with high-quality plant protein sources (legumes, soya, nuts); chicken/poultry/fish; fish only; poultry only; mixed animal protein sources (including dairy); and carbohydrates (low-quality refined grains and simple sugars, such as white bread, pasta, rice, cookies/biscuits). 36 studies with 1803 participants were included and changes in blood concentrations of total, low-density lipoprotein, high-density lipoprotein cholesterol and triglycerides were assessed.
Overall the results show that the impact of red meat consumption on blood lipids depends on the comparator food or diet. This study confirmed that substituting red meat with high-quality plant foods (ie, soya, nuts, and legumes) led to more favourable changes in total cholesterol and LDL-cholesterol concentrations. Interestingly, substituting red meat for fish or fish and poultry did not result in favourable changes to LDL-cholesterol levels although fish did increase HDL-cholesterol levels. Conversely, refined carbohydrates had a worse impact on blood cholesterol than red meat, which is pretty shocking. Impact on triglyceride levels was less apparent when substituting red meat for other protein sources. The exception being that tress nuts, especially walnuts, resulted in favourable changes to all lipid parameters studied.
It’s therefore interesting to consider that the European Society of Cardiology don’t further emphasise the benefits of plant sources of protein, especially nuts, and are wedded to the benefits of fish. In addition, we know that lean meat, including poultry, has a similar impact on blood cholesterol as red meat based on the results of intervention studies. People are often surprised to learn this given dietary recommendations continue to suggest poultry or ‘white’ meat is better for cardiovascular health.
The authors conclude ‘Taken together, these results suggest important potential cardiovascular benefits from replacing red meat with nuts, soya, and other healthy plant foods’. Potential mechanisms include the lower/absent saturated fat and cholesterol in plant foods, higher fibre and unsaturated fat content and the absence of other harmful substances like haem iron and dietary precursors of trimethylamine oxide.

WALNUTS AND CHOLESTEROL: The most studied nut is the walnut. In part due to the California Walnut Commission that has a funded a large number of these studies. The Walnut and Health Aging Study (WAHA) was a randomised, 2-year clinical trial conducted in free-living, cognitively healthy elderly men and women with the primary aim of assessing the impact of walnuts on cognitive health. WAHA is the largest and longest nut trial to date. The intervention group received 30–60g of walnuts per day to supply 15% of energy intake.
The current study reports the impact of walnut consumption on blood cholesterol levels and included 628 participants. The walnut diet significantly decreased total cholesterol LDL-cholesterol and intermediate-density lipoprotein cholesterol (precursor to LDL and refers to a density between that of low-density and very-low-density lipoprotein) corresponding to reductions of 4.4%, 3.6%, and 16.8%, respectively, whereas triglycerides and high-density lipoprotein cholesterol were unaffected. Total LDL particles and small LDL particle number decreased by 4.3% and 6.1%, respectively. It is the small dense LDL particles that have the most adverse impact on cardiovascular health as they are most associated with the development of atherosclerosis. This finding is relatively novel.
Overall, there was a mean reduction of 4.3 mg/dL in LDL-cholesterol and total cholesterol was lowered by an average of 8.5 mg/dL in the intervention group. Of note, the participants had a mostly normal lipid profile at baseline (with 50% of participants on statins). From prior studies, it is predicted that the impact would be greater in those with hypercholesterolaemia and that in people with high triglycerides nut consumption in general has been seen to be beneficial.
A prior report from the WAHA study showed reductions in inflammatory markers in the walnut group, however, the impact on the primary outcome of cognitive decline has been pretty minor and inconclusive to date. It may be that the interventional was too short to observe a beneficial effect. Remarkably, longer observational studies suggest that walnut consumption can positively impact life expectancy. Results from the Nurses’ Health Study and Health Professionals Follow-up study with 18 years of follow-up showed greater life expectancy of 1.78 years in women and 1.94 years in men among those who consumed walnuts more than 5 servings/week, with significant reductions in all-cause and cancer mortality.
The active components of walnuts are thought to be the short chain omega-3 fatty acid alpha-linolenic acid, fibre and gamma-tocopherol, a vitamin E compound. To be honest, most nuts have been found to be benefit health. Last week I wrote about the benefits of pecans for their cholesterol-lowering effects. So, load up on nuts and benefits abound. We have a great new article on our website on nuts and seeds by our member Natalie Peckett, PhD student and 4th year medical student.
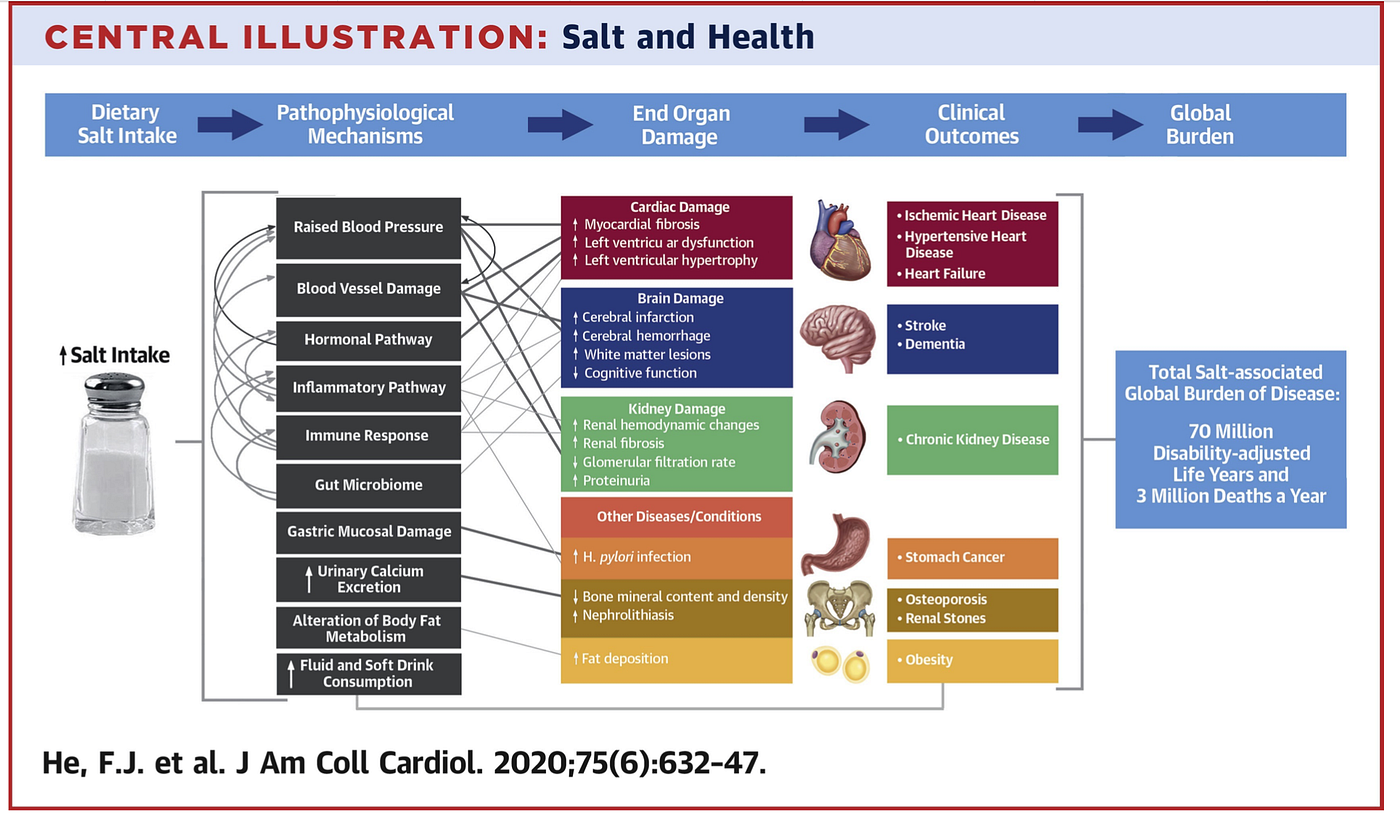
SALT REDUCTION INTERVENTION: Recently there has been some confusion in the medical literature about the impact of salt (sodium chloride) in the diet and it’s impact on health outcomes, particularly CVD. However, overwhelming the scientific data supports salt reduction for improving a number of health outcomes, including CVD. High salt intake was identified as the top dietary risk factor for death globally.
Most of our salt consumption comes from processed and packaged food and that consumed outside of the home. Average salt intake in the UK is around 8g per day when we should actually be aiming for less than 5g a day or even lower.
This unique and ambitious intervention study, the Salt Substitute and Stroke Study (SSaSS), compared the effect of reduced sodium salt substitute versus regular salt on stroke, cardiovascular events, mortality and clinical hyperkalaemia. Participants were adults with either previous stroke or age 60 years and above with poorly controlled blood pressure. The trial was conducted in 600 villages in rural areas of five provinces in China. Approximately 35 individuals were recruited from each village with a total of 20,995 participants. The average age of participants was 65.4 years and 49.5% were female. 72.6% had a history of stroke and 88.4% had a history of hypertension. The villages were randomly assigned in a 1:1 ratio to the intervention group, in which the participants used a salt substitute (75% sodium chloride and 25% potassium chloride by mass), or to the control group, in which the participants continued to use regular salt (100% sodium chloride). 20g of salt per person per day was provided to participants and enough for each member (this seems rather a lot but this included salt used for food preservation).
During an average follow up of 4.74 years there was a 14% reduction in the risk of stroke with the salt substitute compared to regular salt. Major CVD events (non-fatal stroke, non-fatal acute coronary syndrome, vascular death) were reduced by 13% and there was a 12% reduction in mortality. The salt replacement was correlated with significant lowering of systolic, but not diastolic, blood pressure. There was no increased risk of adverse events due to high potassium intake although those at high risk of elevated blood potassium levels were excluded.
This is a pretty remarkable impact of a low-cost intervention. The authors quote it costs about $1.62 per kilogram of salt substitute versus $1.08 per kilogram of regular salt in China.
As highlighted in the image above. Excessive salt consumption has a variety of multi-system adverse effects. Most countries need to address salt intake on a population level. This study demonstrates a possible effective intervention.
IMPACT OF DIETARY PATTERNS ON ALL-CAUSE MORTALITY: Despite discussing individual foods and nutrients in the studies above, its increasingly clear that its more useful for clinical practice to investigate the impact of dietary patterns rather than individual components. This is because ‘nutrient and food analyses cannot account for the interactions among or the degree of independent variation of coingested nutrients and food components’.
The current study was performed by the Dietary Guidelines Advisory Committee convened by the US Department of Agriculture and Department of Health and Human Services and the researchers asked ‘What is the association between dietary patterns consumed and all-cause mortality?’.
The systematic review included 153 articles (involving 6,550, 664 individuals), of which 1 was from a randomised clinical trial and 152 were from observational studies. Of note the randomised study included was the well publicised PREDIMED study, which investigated the impact of a Mediterranean diet intervention for primary prevention of CVD. The majority of the observational studies (72%) examined diet pattern and quality using dietary indices or scores such as the Alternate Healthy Eating Index, Mediterranean diet index and the plant-based diet index. Different diet patterns were also examined including the Mediterranean, Dietary Approaches to Stop Hypertension, vegetarian and vegan and country-specific diet patterns such as the Japanese diet.
The results showed that common features of the dietary patterns associated with improved all-cause mortality were relatively higher intake of vegetables (with or without potatoes); legumes; fruit; nuts; either whole grains specifically, cereals unspecified, or non-refined grains; fish and/or seafood; lean meat or poultry, when meat was included; and unsaturated fats in place of saturated fats; and (2) relatively lower intake of red and processed meat and/or meat and meat products; high-fat dairy; refined grains; added sugars and/or sugar-sweetened beverages; solid fats, saturated fats, and/or trans fat; and excessive sodium. The results were pretty similar regardless of country or diet pattern studied.
Many of the dietary indices considered alcohol consumption in low to moderate amounts or within a threshold (eg, 10–25 g/d; 0.5–1.5 drinks/d for women and 0.5–2.0 drinks/d for men) as a positive factor within a healthy diet pattern.
Interestingly, although not surprising, when adherence to dietary patterns was combined with other healthier lifestyle factors (eg, not smoking and meeting recommended physical activity levels), stronger associations were observed with greater reductions in mortality.
For those interested in plant-based diets, 5 of the included studies examined the impact of diet patterns that avoid animal foods. This included the results from the EPIC-Oxford and Adventist Health Study-2 cohorts. Only two of the studies included demonstrated a benefit for mortality, the Adventist Health Study-2 and results from the Nurse’s Health Study and Health Professionals Follow-up study. In addition, 2 studies showed that greater adherence to the healthy plant-based diet index was associated with lower all-cause mortality. One from the ARIC (Atherosclerosis Risk in Communities) study and one from the US National Health and Nutrition Examination Survey study cohort. I did not see this study, which I reviewed on 22nd August, included. This new study reports further data from the US National Health and Nutrition Examination Survey with more than 40,000 participants and found a reduced risk of all-cause mortality in those most adherence to a healthy plant-based diet.
Overall, the data confirm that nutrient-dense diet patterns characterised by higher intake of vegetables; legumes; fruits; nuts; either whole grains, cereals, or non-refined grains; fish; and unsaturated vegetable oils and by lower or no consumption of animal products (red and processed meat, meat and meat products, and high-fat dairy products), refined grains, and sweets (ie, higher in added sugars) improve longevity and reduce the risk of death from all-causes. On this basis, it can be assumed that a healthy plant-based diet that avoids all animal foods may also be associated with improved longevity but at the moment we don’t have as many studies on 100% healthy plant-based diets to be absolutely certain.
Please follow my organisation ‘plant-based health professionals UK’ on Instagram @plantbasedhealthprofessionals and facebook. You can support our work by joining as a member or making a donation via the website.