An update on nutritional factors and COVID-19, 12th September 2021
It is exactly 2 years since I started writing my weekly updates. This week I bring you an update on the impact of nutrition on COVID-19 as I prepare for my talk at Global VegFest on 18th September. Hope to see you there!
On March 14th, just prior to the first lockdown in the UK, I wrote an article summarising the dietary and lifestyle factors that are important in maintaining a healthy immune system. I highlighted the role of certain nutrients, including flavonoids, vitamin C, selenium and zinc. I discussed the importance of adequate vitamin D intake and maintaining a healthy gut microbiome. I concluded that a diet focussed on whole plant foods and minimising animal-derived and processed foods is associated with better health and a more robust immune system.
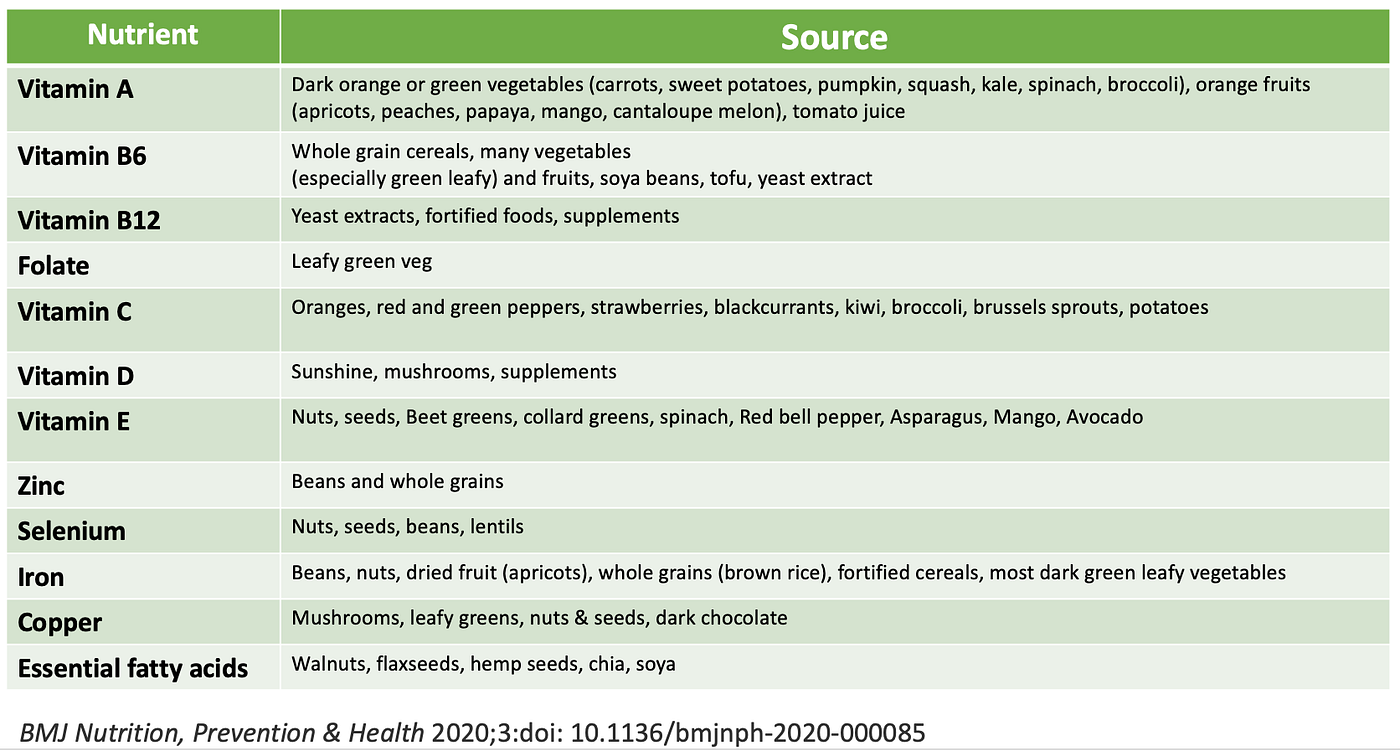
At the start of the pandemic a number of papers and review articles were published in the scientific literature summarising the impact of diet and lifestyle on the health of the immune system. Many physicians, researchers and scientists advocated for healthy diets as part of the approach to pandemic resilience. The table below lists the nutrients we know to be important for maintaining a healthy immune system in the context of a healthy diet pattern.
I provided an update on emerging research on nutritional factors and COVID-19 on Sept 27th 2020. This current article builds on the prior one so please do refer back to it. A year on, we are now more certain about the positive role a healthy, plant-based diet can play in reducing the impact of the pandemic virus that causes the disease COVID-19.

COVID-19 AND UNDERLYING HEALTH CONDITIONS: We knew early on in the pandemic that those with underlying health conditions had a greater risk of hospitalisation and death once infected with SARS-CoV-2. This large study from the US analysed nearly 1 million hospitalisations and found that 60% of the attributable risk was due to 4 underlying conditions; obesity, hypertension, heart failure, type 2 diabetes. In simple terms, this means that if those four conditions did not exist, then 60% of hospitalisations would have been avoided.
A similar type of study published from the UK in the first wave of the pandemic analysed more the 17 million GP records and linked the data with over 10,000 COVID-19 related deaths. The results showed that more than 90% of people who died had at least one underlying chronic health condition, with obesity, cancer, renal failure, type 2 diabetes, chronic respiratory and heart conditions and conditions that impair the function of the immune system, predicted for a higher risk of death from COVID-19.
Many of these underlying chronic conditions can be prevented and modified by adopting a healthy plant-based diet and lifestyle. We must not forget though that there are also some risk factors that can not be modified such as age and male sex and some that can not easily be modified in the short term but are equally important to address, including socioeconomic status and racial disparities.
Unfortunately, studies have shown that on average, body weight in both adults and children has increased during the pandemic, certainly in high income countries. In US adults, body weight increased by 1.5Ibs per month. In US children, there was an increase of 2.3kg above that expected for gains in height between March 2020 and January 2021. Changes in lifestyle habits have varied with some studies finding positive changes, buying more fresh produce and cooking at home, and others negative changes, less physical activity and increased consumption of processed foods. I in 3 adults in the UK increased their alcohol consumption.

COVID-19 IS A VASCULAR DISEASE: The endothelium is the single cell layer covering the inside of the 60,000 miles of blood vessels in our body. This layer of cells maintains the health of blood vessels but also plays a crucial role in maintaining the normal functions of the body, including the immune system, inflammation and coagulation pathways. Endothelial cells release substances that control vascular relaxation and contraction as well as enzymes that control blood clotting, immune function and platelet adhesion. SARS-CoV-2 enters cells by attaching to the ACE2 receptor, which is abundant on endothelial cells and thus a target of the virus. The downstream effects of this are clinical manifestations such as loss of smell, COVID toe, inflammation of the heart and its lining, thrombosis, immune dysregulation and of course the well-recognised acute respiratory distress syndrome.
The underlying conditions that predict for a worse outcome with SARS-CoV-2, such as hypertension, heart failure, renal failure and type 2 diabetes, are all characterised by endothelial dysfunction and thus it is highly plausible that the virus’s ability to further disrupt endothelial function is the reason why these conditions predict for a worse outcome.
DIET AND ENDOTHELIAL HEALTH: Diet and lifestyle factors are important in maintaining endothelial health. One crucial factor in maintaining endothelial health is a ready supply of nitrous oxide (NO), which controls vascular tone and maintains the integrity of this layer of cells. In addition, a constant supply of antioxidants from food is crucial to counteract the effect of free radicals that contribute to endothelial injury.
This hypothesis generating review highlights the potential impact of a healthy diet and lifestyle in maintaining vascular health and preventing endothelial dysfunction. Plant foods, including herbs and spices, are high in antioxidant compounds that help protect against the damage caused by free radicals. The article reviews the general benefits of consuming nitrate-rich vegetables, mainly leafy greens and beetroot. Prior studies have shown that the consumption of nitrate-rich green leafy vegetables, maybe as little as a cup a day, could significantly reduce the risk of cardiovascular diseases such as hypertension, ischaemic heart disease, heart failure, ischaemic stroke and peripheral artery disease. A systematic review and meta-analysis of 34 studies found that dietary nitrates significantly reduce resting blood pressure, improve endothelial function, reduce arterial stiffness and reduce platelet aggregation. Randomised studies of beetroot juice have confirmed its ability to reduce blood pressure as effectively as prescribed medications. In addition, beetroot juice consumed before an athletic event may enhance performance.
Although the paper highlighted is entirely hypothesis generating and there are no clinical trials demonstrating an impact of nitrate-rich vegetables on COVID-19 outcomes, there is logic to the argument based on prior knowledge of the role of diet in maintaining endothelial health.
CHOLESTEROL AND COVID-19: COVID-19 disease requires SARS-CoV-2 to enter the cells. It does this mainly through binding of the viral spike protein to the receptor ACE2 on the surface of cells. There are certain factors and conditions that will increase the level of ACE2 on cells and hence enhance entry of the virus into the cells.
This paper (currently as a pre-print) highlights how cholesterol loading of cells and cell membranes is a key factor in facilitating entry of the virus into the cells and enhancing the infectivity of the virus. This is supported by the observational studies that have shown that prior use of statin medications may reduce the severity of COVID-19.
Now of course, these studies are referring to cholesterol inside the cells, which is different from the cholesterol that is measured by blood tests. However, there is a general correlation between higher blood cholesterol and tissue cholesterol and certainly high blood lipids contribute to vascular damage and increase the risk of cardiovascular diseases. In people with high blood cholesterol, overtime, this will accumulate in various cells, including those in the lung and immune cells, such as macrophages. Conditions such as obesity and type 2 diabetes are also associated with higher cellular cholesterol. Thus, maintaining healthy blood lipid levels is a useful approach to reducing the the severity of SARS-CoV-2 infection. A plant-based diet is the easiest, most effective way to keep blood cholesterol at healthy levels.

HIGH BLOOD GLUCOSE AND COVID-19 SEVERITY: A number of observations have been made about blood glucose levels and COVID-19. People with type 2 diabetes are at higher risk of severe disease, most patients admitted to the intensive care unit (ICU) with COVID-19 have high blood glucose levels and there is an increased risk of developing type 2 diabetes after COVID-19 infection.
This novel paper made use of a machine learning tool to mine data from 240,000 open access, scientific articles. The authors used the machine learning algorithms to look for patterns and trends in results of studies that investigated the role of blood glucose in COVID-19 severity. The researchers found that elevated blood glucose facilitates virtually every step of the SARS-CoV-2 infection. Elevated blood glucose increases glucose in the pulmonary airway surface liquid, which impairs the immune defences of the lungs. It facilitates binding of the virus to the ACE2 receptor and hence entry into the cells and then further replication of the virus. Elevated blood glucose impairs the function of immune system and increases the risk of an exaggerated response leading to cytokine storm and acute respiratory distress syndrome. In addition, elevated glucose levels increase the risk of multi-organ failure and thrombotic events.
Unfortunately, this paper goes on to hypothesise that restricting carbohydrate in the diet may be a way to reduce blood glucose levels. This may be relevant for people admitted to ICU who require artificially feeding. For the rest of us, the best approach for regulating blood glucose is by eating a fibre-rich plant-based diet.
FATTY LIVER DISEASE AND COVID-19: Overweight and obesity is a risk factor for a more severe illness with the SARS-CoV-2 virus. This study investigated whether fatty liver disease, often, but not exclusively, associated with obesity, is an independent risk factor for severe COVID-19.
The retrospective study included participants from the UK Biobank study of whom 41,791 underwent MRI (aged 50–83) for assessment of liver fat, liver fibro-inflammatory disease, and liver iron. Positive COVID-19 test was determined from UK testing data, starting in March 2020 and censored in January 2021. 4,458 had a COVID-19 test result available with 1,043 testing positive and 3,415 testing negative. Thirty-two (3.1%) patients who tested positive were hospitalized either 1 week or 1 month after the positive test result. These patients were mostly male and had significantly higher BMI and liver fat compared to other positive patients who did not require hospitalization. The 8 patients were admitted to intensive care had significantly higher liver fat, liver inflammation and BMI compared to all other positive participants who did not require intensive care. Even after a multi-variate analysis with other risk factors, including, age, male gender, non-Caucasian ethnicity, lower socio-economic class and high BMI, fatty liver disease remained a risk factor for more severe disease. Overall, having severe fatty liver disease of greater or equal to 10% was found to be a significant risk factor for testing positive for COVID-19 and hospitalisation. Those participants with fatty liver disease defined by liver fat ≥10% and BMI ≥ 30 Kg/m2 were 5.14 times more at risk of being hospitalised with severe disease. This equate to around 11% of the UK population being at risk.
The mechanisms by which fatty liver leads to more severe disease still needs to elucidated and of course the numbers with severe COVID-19 in this study were very small. In the meantime the authors conclude that the results highlight the ‘importance of “de-fatting” the liver to reduce susceptibility’. The good news is that a healthy diet and lifestyle habits are very effective at preventing and reversing fatty liver. I have summarised this topic frequently. Below is the evidence-based approach for prevention and reversal of fatty liver.
- Calorie restriction with a 500–1,000 kcal daily deficit is an extremely effective lifestyle intervention for both the prevention of NAFLD and histological improvement in patients with established disease. The goal of calorie reduction should be to achieve ≥10% overall body weight loss.
- Reduce intake of red and processed meats
- Reduce/eliminate refined carbohydrates and especially fructose
- Increased fibre intake through the consumption of fruits, vegetables, whole grains and legumes
- Replace dietary saturated fatty acids with mono-unsaturated and poly-unsaturated fatty acids
- Coffee consumption is protective against the development of NAFLD and disease progression. Moderate to heavy alcohol consumption should be avoided in the presence of obesity, NAFLD, and other metabolic risk factors. Abstinence is advised for patients with advanced fibrosis.

GUT MICROBIOME AND SEVERITY OF COVID-19: Initially it was thought that SARS-CoV-2 was mainly a respiratory illness, but it soon became clear that the virus has an impact on several organs, including the gut. Not only is the viral receptor ACE2 expressed in the gut, contributing to gastrointestinal symptoms, it has become apparent that the composition of the gut microbiome is associated with the severity of the infection. We also know that there is communication between microbes in the gut and the lung — the gut-lung axis.
This paper from China analysed the composition of the gut microbiome and measured blood markers of inflammation in 100 hospitalised patients with COVID-19 and compared the results to 78 healthy volunteers. Serial stool samples were collected from 27 of the 100 patients up to 30 days after clearance of SARS-CoV-2.
The study found that patients with COVID-19 had significant alterations in the composition of the gut microbiome, including reductions in Faecalibacterium prausnitzii, Eubacterium rectale and several bifidobacterial species that are known to regulate the immune response. These strains of bacteria thrive on dietary fibre and are important in producing short chain fatty acids, which reduce inflammation and regulate the immune system. The study showed that the greater the change in the composition of the gut microbiome the more severe the inflammatory response as determined by the levels of inflammatory markers in the blood. These changes in the microbiota persisted after clearance of the virus. The authors conclude ‘Bolstering of beneficial gut species depleted in COVID-19 could serve as a novel avenue to mitigate severe disease, underscoring importance of managing patients’ gut microbiota during and after COVID-19‘. The authors hypothesize that these persistent changes in the microbiome composition could contribute to the persistence of symptoms after recovery from COVID-19.
Of course there are several limitations to this study. It only includes a small number of patients, many patients received antibiotics as part of their treatment, the changes in the gut microbiome may just be a reflection of the underlying health status of the individual rather than having a causal relationship to the SARS-CoV-2 infection itself. Nonetheless, the gut microbiome is easily modified by healthy lifestyle habits, including a fibre-rich plant-based diet. Previous studies have linked the consumption of cruciferous and fermented vegetables, known to be beneficial for gut health, with a reduced risk of death from COVID-19.
VITAMIN D AND COVID-19: Vitamin D is a steroid hormone that is lipid soluble and can enter cells and nuclei altering gene transcription. Vitamin D receptors are found throughout the body and affects the function of a number of cells, including immune cells. We had data prior to the pandemic to support the role of vitamin D supplementation in reducing the risk of acute respiratory infections.
There has been much discussion about the impact of vitamin D deficiency on the risk of COVID-19 and it’s severity. Although data have not been consistent, the UK Government recommended vitamin D supplementation for all citizen during the periods of lockdown when sunshine exposure was inadequate.
The paper highlighted is a meta-analysis of 14 studies that assessed the association between vitamin D levels and the risk of COVID-19 infection. The results showed that individuals with vitamin D deficiency were at 80% increased risk of COVID-19 infection compared to those whose vitamin D levels were sufficient.
A pre-print article brings together the results of 4 intervention studies assessing the impact of vitamin D supplementation on outcomes for patients with COVID-19. A total of 259 individuals (140 females and 119 males) were included in the analysis with 139 allocated to the intervention groups. The results suggest that supplementation could reduce the severity of COVID-19 and mortality. This is a very small study and no firm conclusions can be made with more information needed on the dose and duration of supplementation. Nonetheless, the data we have so far suggests at the very least that we should all be aiming for a vitamin D level within in the normal range and if it is not, then supplementation would be appropriate, especially given the lack of side effects at doses less than 4000IU per day.
DIET PATTERNS AND COVID-19: Eighteen months into the pandemic we had the first study supporting a dietary approach to reducing COVID-19 severity. The paper highlighted reports the results of a case-control study of healthcare workers, mostly physicians, with significant exposure to COVID19 patients from 6 countries. Participants completed a web-based survey from 17 July to 25 September 2020. Information was collected on basic demographic characteristics, past medical history, medications, lifestyle, and COVID-19 symptoms, and a 47-item food frequency questionnaire. The questions captured the dietary patterns of participants over the prior 1 year and included 11 choices; whole foods, plant-based diet; keto diet; vegetarian diet; Mediterranean diet; pescatarian diet; Palaeolithic diet; low fat diet; low carbohydrate diet; high protein diet; other; none of the above. For the analysis ‘whole foods, plant-based’ diets and ‘vegetarian’ diets were placed into one category called ‘plant-based diets’, n=254. For the pescatarian diet, data were combined from those following a whole foods plant-based, vegetarian and pescatarian diets, the latter only being 40 participants (n=294). The study included 568 COVID19 cases and 2316 controls. Those participants who had had COVID19 were asked to rate the severity based on 5 options from very mild to critical, requiring intensive care.
The results showed that those following a plant-based diet pattern had a 73% reduction in the risk of moderate or severe COVID19 and those following a pescatarian diet had a 59% reduction in risk. This was independent of BMI and underlying chronic health conditions. In contrast, participants following a high protein, low carbohydrate diet had a 3-fold higher odds of moderate or severe COVID-19 when compared to the plant-based group.
We do have to accept the major limitations of this study when extrapolating these results to a healthy plant-based or vegan diet. This was not a study of people following a vegan or 100% plant-based diet, despite the media headlines suggesting the contrary. In fact, those classified as plant-based were not that healthy, consuming a median of 3.7 portions of legumes and 9.8 portions of fruits per week and still consuming some animal foods, including similar amounts of dairy and eggs to the non-plant-based group, and similar amounts of refined grains. However, their consumption of legumes, nuts and vegetables was significantly higher and consumption of red/processed meat, sugar-sweetened beverages and alcohol significantly lower than those participants who did not follow a plant-based diet.
Furthermore, this is not a robust study design being a case-control study, with self-reported dietary data and no set definition of low-carb or plant-based. In addition, COVID-19 infection was based on symptoms rather than validated test results. The impact of residual confounding can not be excluded and people with more severe COVID-19 may not have been able to participate. In addition, the participants were mainly male, Caucasian physicians.
PLANT-BASED DIETS AND RISK AND SEVERITY OF COVID-19: This paper reports results from the now famous Zoe COVID symptom study. The study analysed diet quality in more than half a million participants from the US and UK. During the follow-up period, 31,815 COVID-19 cases were documented. Adherence to a healthy plant-based diet was calculated using the healthy plant-based diet index which gives positive marks to healthy plant foods and negative marks to unhealthy plant foods and all animal foods. Those eating a healthy plant-based diet as defined by the healthy plant-based diet index had a 10% reduction in risk of getting COVID-19 and a 40% reduction in getting severe disease. The impact of a healthy diet was greatest in those from lower socioeconomic groups and independent of underlying chronic health conditions, body mass index, smoking and physical activity.
Based on these results, it was calculated that nearly a quarter of COVID-19 cases could have been prevented if these differences in diet quality and wealth had not existed.
Of course, this is not a perfect study. It is observational with self-selected participants, self-reported dietary information and for the primary outcome of COVID-19 infection, a validated symptom-based algorithm was used rather than PCR test results. However, this is likely to be the best evidence we can expect to have outside of a randomised study.
There are a number of reasons why a plant-based diet may have shown these advantages. It’s anti-inflammatory and anti-oxidant properties, the ability to maintain a healthy gut microbiome and hence healthy immune system and the reduction in underlying healthy conditions (although the results were adjusted for this). Even though the theory is obvious, it is great to see real life applicability in the setting of an infectious threat
The authors conclude ‘Our data provide evidence that a healthy diet was associated with lower risk of COVID-19 and severe COVID-19 even after accounting for other healthy behaviours, social determinants of health, and virus transmission measures’
UNINTENDED CONSEQUENCES OF COVID-19: The pandemic has reminded us that the meat industry not only harms non-human animals but also humans that work within it. Early in the pandemic we learnt that slaughterhouse and meat workers were at high risk of contracting SARS-CoV-2 infection due to the nature of their working conditions. In the US, these approximately half a million workers were classed as essential and had little choice but to continue working, often being from migrants or refugee communities.
This paper examines county-level rates of COVID-19 in the US and whether the presence of large meat-packing plants have an impact on the rates of infection. The study finds that within 60 days after the emergence of COVID-19 in a given county, the presence of a meat packing facility increased per capita infection rates by 110–160% compared to counties without packing plants. This translated into 334, 000 COVID-19 cases being attributable to large meatpacking operations. This estimate includes both direct infections to meatpacking workers as well as community spread outside the operations but attributable to those facilities.
The study finds that previous reports have underestimated the impact of meat packing plants on COVID-19 case rates and also believes their estimates are likely to have missed cases too. For example, if the worker contracted COVID-19 at work but lived outside the county and transmitted it to his/her community, these cases would not have been attributed to the meat packing plant.
The authors conclude ‘that the COVID-19 mortality and morbidity associated with large packing plants has generated more than $11.6 billion in economic costs to the rural economy with beef and pork facilities’.
Given that meat consumption is not essential, the harm caused to meat packing workers and their families is unforgivable and violates human rights. If we ourselves could not work in such a facility then we should not expect our fellow kin to do so on our behalf.

PANDEMIC RESILIENCE: This superb editorial sums up nicely our current knowledge and puts out a call to action; ‘It seems clear from the data available that nutrition is one of the keys to global pandemic resilience, both for the current and future pandemics and could reduce burdens on healthcare systems. Optimal nutritional status is a defence against both communicable and non-communicable diseases. It is also something that can be attended to right now and is not months away. We are ecological creatures at a crossroad — let this pandemic be your wakeup call’.
Please follow my organisation ‘plant-based health professionals UK’ on Instagram @plantbasedhealthprofessionals and facebook. You can support our work by joining as a member or making a donation via the website.