An update on nutritional factors and COVID-19, 24th April 2022
This week I bring you up to date on diet, immunity and COVID-19. No surprises that studies continue to support the benefits of a plant-based diet, a healthy gut microbiome and adequate vitamin D.
I have been following with great interest the studies on diet, nutrition and COVID-19 outcomes. My previous summary articles can be found here (make sure you scroll down for recent updates). To date, we have learnt that a healthy diet is key to maintaining physical and mental well-being during the pandemic, diet and lifestyle-related chronic conditions worsen outcomes and increase the risk of death with COVID-19. High cholesterol, high blood glucose along with poor vascular health enhances the viruses’ ability to cause damage to cells, blood vessels and organ function. The health of the gut microbiome is associated with severity of infection and a healthy plant-based diet may be a useful tool for reducing the impact of the pandemic virus. Here are some more studies emphasising these findings.
NUTRITION AND IMMUNITY: This review provides an excellent overview of the impact of nutrition on the immune system. When it comes to infections, the immune system has four main functions. It acts as a barrier to stop pathogens entering the body; it can recognise whether micro-organisms are harmful or not; it can act to eliminate harmful micro-organisms; it forms a memory so that it can respond more quickly should it encounter the same pathogen in the future.
There are many potentially modifiable factors that affect the functioning of our immune system including stress, physical fitness, frailty, body fatness and diet. Diet specifically has a number of influences on the immune system. Diet provides the building blocks for the generation of RNA, DNA, production of proteins (antibodies, cytokines, receptors, acute phase proteins etc.) and new cells. It provides specific substrates for the production of immune-active metabolites (e.g. arginine as a substrate for nitric oxide). It provides regulators of immune cell metabolism (e.g. vitamin A, zinc) and nutrients with specific anti-bacterial or anti-viral functions (e.g. vitamin D, zinc). Diet provides nutrients that protect the host from oxidative and inflammatory stress (e.g. vitamin C, vitamin E, zinc, selenium, long-chain omega-3 fatty acids and many plant polyphenols) and substrates for the intestinal microbiota which in turn modulates the immune system. The table below summarises the key nutrients required for a healthy immune system and their food sources.
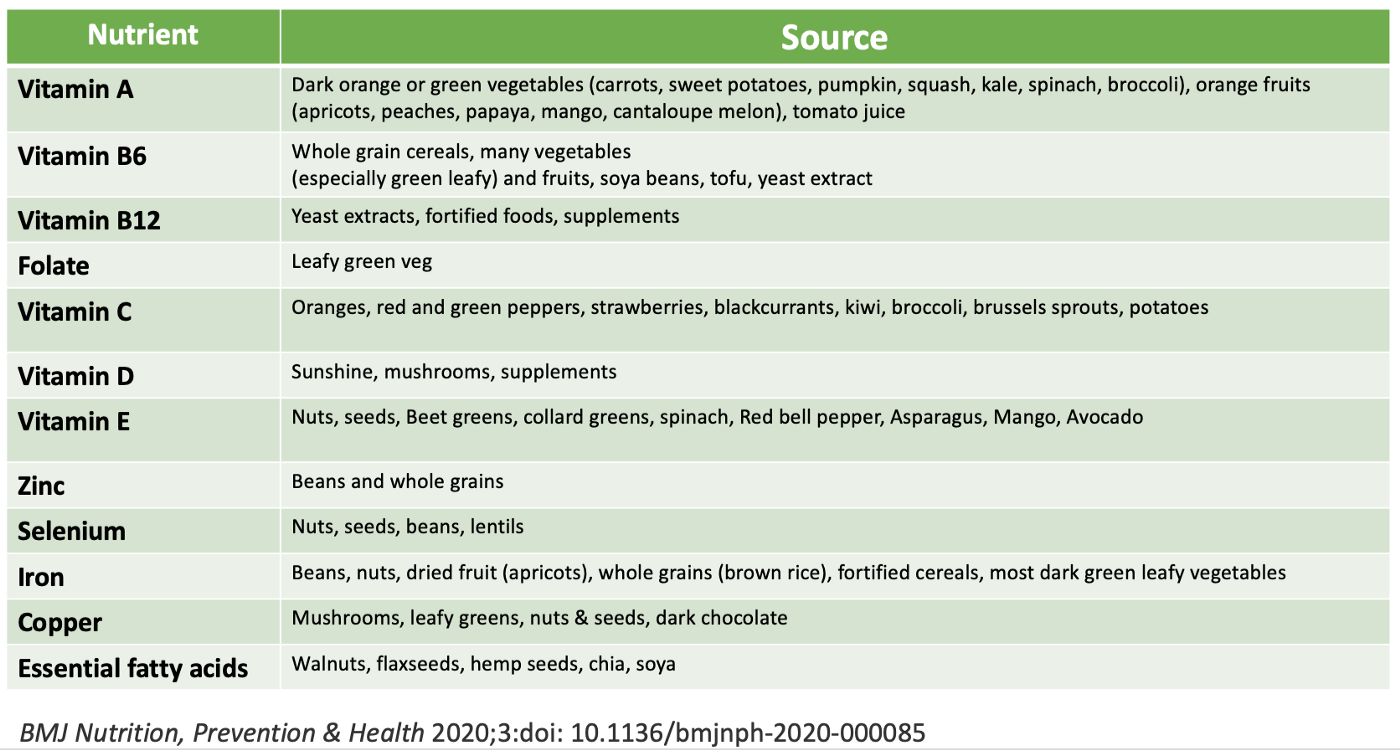
The review reminds us about the importance of ‘addressing the current nutritional inadequacies (frailty, obesity, general undernutrition, micronutrient insufficiency or deficiency) that are widespread in the population in order to better support the immune response. This is the major lesson from the study of nutrition and immunity that is relevant for the battle with SARS-CoV-2 and the disease it causes, COVID-19, and for ensuring the population is better prepared for future pandemics’.

GUT MICROBIOME AND COVID-19 OUTCOMES: A healthy gut microbiome is key to the optimal functioning of the immune system. Bacteria within the gastrointestinal (GI) tract create a barrier protecting against colonisation by pathogens and can directly inhibit the growth of pathogens, through the production of lactic acid and antimicrobial proteins. The gut microbes also interacts with the gut epithelium (lining of the gut wall) and the associated immune cells. Communication between the gut bacteria and the immune system occurs through both direct contact and through chemicals released from the bacteria. Beneficial bacteria thrive on fibre and polyphenols derived from plant foods. These nutrients are required to make short chain fatty acids, which are used to communicate with cells in the gut but also to immune cells in distant organs including the lung i.e. the gut-lung axis.
A study from China analysed the composition of the gut microbiome and measured blood markers of inflammation in 100 hospitalised patients with COVID-19 and compared the results to 78 healthy volunteers. Serial stool samples were collected from 27 of the 100 patients up to 30 days after clearance of SARS-CoV-2.
The results showed that patients with COVID-19 had significant alterations in the composition of the gut microbiome, including reductions in Faecalibacterium prausnitzii, Eubacterium rectale and several bifidobacterial species that are known to regulate the immune response. These strains of bacteria thrive on dietary fibre and are important in producing short chain fatty acids, which reduce inflammation and regulate the immune system. The study showed that the greater the change in the composition of the gut microbiome the more severe the inflammatory response as determined by the levels of inflammatory markers in the blood. These changes in the microbiota persisted after clearance of the virus. The authors conclude ‘Bolstering of beneficial gut species depleted in COVID-19 could serve as a novel avenue to mitigate severe disease, underscoring importance of managing patients’ gut microbiota during and after COVID-19‘.
This more recent prospective cohort study from Hong Kong investigated whether the gut microbiome contributes to persistent symptoms after the initial acute phase, defined as at least one persistent symptom 4 weeks after clearance of the SARS-CoV-2 virus. 106 people with confirmed COVID-19 were included and compared to 68 matched controls who had not had the infection. Stool samples were analysed at admission to hospital and 1 and 6 months following discharge (at the time of the study all infected patients were admitted to hospital). The gut microbiota profile of those with and without persistent symptoms was compared. The commonest post infection symptoms were fatigue, poor memory and hair loss.
The results showed that people who developed post infective persistent symptoms had a distinct gut microbiota profile on admission to hospital. There was a statistically significant association with certain gut bacteria with higher levels of Ruminococcus gnavus, Bacteroides vulgatus and lower levels of Faecalibacterium prausnitzii. Persistent respiratory symptoms were correlated with opportunistic gut pathogens, and neuropsychiatric symptoms and fatigue were correlated with nosocomial (originating in hospital) gut pathogens, including Clostridium innocuum and Actinomyces naeslundii. This gut dysbiosis persisted at 6 months post infection. Hair loss was associated with the loss of butyrate-producing bacteria whereas those without persistent symptoms at 6 months had a greater abundance of butyrate-producing bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii. In addition, there was an abundance of multiple bacteria known to be beneficial to immune health in those without persistent symptoms. The authors conclude ‘altered gut microbiome composition is strongly associated with persistent symptoms in patients with COVID-19 up to 6 months after clearance of SARS-CoV-2 virus. Considering the millions of people infected during the ongoing pandemic, our findings are a strong impetus for consideration of microbiota modulation to facilitate timely recovery and reduce the burden of post-acute COVID-19 syndrome’.
The good news is that a fibre-rich, polyphenol-rich plant-based diet is associated with better gut health and an abundance of bacteria that produce butyrate and other short chain fatty acids, which are essential for immune health and reduction of inflammation.

PROBIOITCS AND COVID-19: The natural next step is to wonder whether probiotic use could have a beneficial impact. In this randomised study, 300 adult participants of Hispanic orgin with symptomatic COVID-19 in the outpatient setting were included. They were randomly assigned to receive a probiotic supplement or placebo. The active product (AB21© probiotic formula) consisted of capsules containing Lactiplantibacillus plantarum KABP033 (CECT30292), L. plantarum KABP022 (CECT7484), L. plantarum KABP023 (CECT7485) and Pediococcus acidilacticiKABP021 (CECT7483), in a ratio of 3:1:1:1 colony- forming units (CFU), respectively, and a total dose of ≥2×109 total CFU, with a maltodextrin carrier. The impact of the probiotics on complete symptomic and viral remission (negative PCR test) was assessed.
Patients were enrolled within 7 days of the onset of symptoms and COVID-19 was confirmed by a PCR test. Participants took one probiotic tablet (four strain composition) prior to breakfast for 30 days. They were assessed on day 0, 15 and 30 of the study. Participants were also contacted by phone on days 5, 10 and 20. Nasopharyngeal, blood and faecal samples were collected and analysed and chest x-rays were performed. Participants were only allowed to use paracetamol as an additional medication.
During the study there were no hospitalisations or deaths. Probiotic supplementation was well-tolerated and reduced nasopharyngeal viral load, lung infiltrates and duration of both digestive and non-digestive symptoms, compared to placebo. The primary outcome of complete remission (i.e. complete symptomatic and viral clearance) on day 30 was achieved by 78 (53.1%) in the probiotic group compared to 41 (28.1%) in placebo. No significant compositional changes were detected in faecal microbiota between the probiotic and placebo groups, but probiotic supplementation significantly increased specific IgM and IgG against SARS-CoV2 compared to placebo. The authors hypothesise that this probiotic primarily acts by interacting with the host’s immune system rather than changing colonic microbiota composition.
Although these results are unlikely to influence clinical practice right away, the results support prior evidence that shows a healthier gut microbiome is important for improving outcomes from COVID-19.
PHYTO-RICH, PROBIOTIC CAPSULE FOR COVID-19: This study from the UK tested whether a combination of phytonutrients and probiotics could improve symptoms of COVID-19 infection. 147 participants with symptomatic COVID-19 were randomised to receive a placebo (P) or a phytochemical-rich concentrated food capsule (PC) in addition to a pre/probiotic lactobacillus/inulin capsule for 30 days. Phytochemical-rich whole food capsule contained: Citrus Sinensis fruit (400 mg from 200 mg of 2:1 extract, standardised to contain 70 mg of Bioflavonoids). Chamomile, Matricaria recutita L. flower) (1000 mg from 22 mg of 10:1 extract and 65 mg of 12:1 extract). Curcuma Longa rhizome in Curcumin Complex (1600 mg of curcumin from 25 mg of 64:1 extract, standardised to contain 23.8 mg of curcuminoid). Pomegranate (Punica granatum L. rinds and seeds) (1000 mg from 25 mg of 40:1 extract, standardised to contain 10 mg of Ellagic Acid). Polygonum cuspidatum root containing 100 mg of resveratrol.
The average time from COVID-19 diagnosis to trial entry was 108 days (range 2 to 467 days). Thirty-six participants (25%) entered the study within 30 days of diagnosis (average 14 days) and 112 (75%) after 30 days (average 120 days). Due to poor recruitment and participants not wanting to only receive placebo, the study protocol was amended such that most of the control group received the probiotic capsule too.
At baseline, the most common symptoms reported were fatigue, shortness of breath, pains, altered sense of smell and bowel symptoms. The results showed that participants taking the PC had an almost two-fold reduction in fatigue scores, a three-fold reduction in cough score and more than a double improvement in overall well-being scores compared to the placebo group. These results were statistically significant. Two (1.5%) participants reported mild, increased bloating which they felt was attributable to the capsules, although GI symptoms improved in 25 of 31 participants (82%) who reported them at baseline. In the subgroup analysis, participants admitted to hospital had a greater improvement after this intervention compared with non-hospitalised participants, which may be a reflection of greater disruption of the gut microbiome.
Although the impact of this intervention was modest and further studies are required, the conclusions are eminently sensible; ‘Although it is still not known whether the benefits seen in this study could have been achieved with determined dietary manipulation alone, in this current pandemic, it would be wise to emphasise food with higher phytochemical content and lifestyle and nutritional factors which are associated with a more favourable gut microbiome’. In other words, a variety of healthy plant foods.

VITAMIN D LEVELS AND SEVERITY OF COVID-19: We have heard a lot about the role of vitamin D in maintaining the health of the immune system during the COVID-19 pandemic, yet whether low blood levels play a causal role in the severity of infection remains to be determined. This study tries to assess the strength of this relationship by assessing the association between pre-infection serum vitamin D levels and disease severity and mortality.
Conducted in Israel, this retrospective study included 253 patients with a mean age of 63 years admitted to hospital with COVID-19 who had pre-infection levels of vitamin D available. The pre-infection levels were divided into divided four categories; deficient, insufficient, adequate, and high-normal. 133 (52.5%) had a level less than 20 ng/mL, 36 (14.2%) had 20 to less than 30 ng/mL, 44 (17.3%) had 30 to less than 40 ng/mL, and 40 (15.8%) had 40 ng/mL or greater. Based on the pre-infection values, patients with vitamin D deficiency (<20 ng/mL) were 14 times more likely to have severe or critical disease than patients with vitamin D levels of >40 ng/mL. There was a progressive decrease in levels of vitamin D as the disease severity increased. Both age and pre-infection vitamin D levels were found to be independent predictors of increased disease severity yet the association with vitamin D levels was demonstrated in all age groups (<50, 50–64, >65 years). The authors conclude ‘The use of historical results obtained before the COVID-19 pandemic as part of a public health survey enabled us to suggest vitamin D deficiency contributes to the causal pathway of COVID-19 mortality risk and disease severity’.
Of course we would prefer prospective or randomised studies to be more certain of this association but in the meantime there are plenty of reasons to make sure your vitamin D levels are in the adequate range and to appropriately supplement to ensure this is maintained. This is relevant to all diet patterns, not just plant-based diets.

DIETARY SUPPLEMENTS AND COVID-19: It is tempting to reach for nutritional supplements to ‘boost’ the immune system and there are compelling data on certain nutrients such as flavonoids, including quercetin, zinc and curcumin. However, the real life experience appears less impressive. The study highlighted reports data from the largest observational study on the topic, the ZOE COVID symptom study, and include 445, 850 participants who reported their use of supplements during the first 3 months of the first wave of COVID-19. The results showed significant association between users of omega-3 fatty acid, probiotic, multivitamin or vitamin D supplements and lower risk of testing positive for infection with SARS-CoV-2 (9-14% lower risk). Of note, this benefit was only in women, but 70% of the participants were women. Supplementing with vitamin C, garlic or zinc did not appear to be of benefit.
A further systematic review and meta-analysis specifically addressed the therapeutic impact of vitamin C, zinc and Vitamin D supplementation. The study included 26 studies (10 randomised controlled trials and 16 observational studies) involving 5633 patient with COVID-19. The results failed to observe a benefit for vitamin C and zinc supplementation although vitamin D supplementation may be associated with lower requirement for a ventilator and shorter length of hospital stay.
BROADER CONCLUSIONS AND LEARNING: It must not be forgotten that our diet choices will determine the risk of future pandemics. Most new and emerging infections are caused by the use of animals as food and the destruction of their natural habitats. The biggest contributor to habitat destruction and species loss is animal agriculture. If we continue consuming meat and dairy, most of which is produced in factory farms, more pandemic infections are inevitable. In the words of the scientists that have sounds the alarm and warned that we are accelerating towards the sixth mass extinction event, ‘There is time, but the window of opportunity is almost closed. We must save what we can, or lose the opportunity to do so forever. There is no doubt, for example, that there will be more pandemics if we continue destroying habitats and trading wildlife for human consumption as food and traditional medicines. It is something that humanity cannot permit, as it may be a tipping point for the collapse of civilization. What is at stake is the fate of humanity and most living species. Future generations deserve better from us’.
PANDEMIC RESILIENCE: This superb editorial, now more than 18 months old, sums up nicely our current knowledge and puts out a call to action; ‘It seems clear from the data available that nutrition is one of the keys to global pandemic resilience, both for the current and future pandemics and could reduce burdens on healthcare systems. Optimal nutritional status is a defence against both communicable and non-communicable diseases. It is also something that can be attended to right now and is not months away. We are ecological creatures at a crossroad — let this pandemic be your wakeup call’.
Please follow my organisation ‘plant-based health professionals UK’ on Instagram @plantbasedhealthprofessionals and facebook. You can support our work by joining as a member or making a donation via the website.